
The lowdown on lower facial rejuvenation

Demand for rejuvenation and contouring of the lower facial third has become increasingly popular in recent years. While some seek enhancement of the jawline and chin for beautification purposes, many seek treatment due to the fact they are concerned about the signs of ageing in this area including bone resorption and loss of supporting structures, loss of volume and tissue elasticity, excess subcutaneous fat or a “double chin” and the formation of jowls.
As techniques to lift and contour the lower face have evolved so too has demand for treatments among both male and female patients. Lower facial contouring has also become one of the fastest growing trends in the East Asian community, due to cultural ideals of beauty.
The youthful lower third
When we talk about lower face contouring the first question that comes to mind is, “Is there any ideal lower face?” One of the major concerns many people have regarding the lower face as they age are jowls. Patients come into clinic complaining that they look sad or “down-faced”. Jowls form as we age for a number of reasons. The underlying structures which support the skin and hold it up begin to deteriorate and at the same time our skin thins and loses its elasticity.
Another factor as we age is that we tend to lose definition under our chins due to excess submental fat, known as the “double chin”, which is more prominent with age.
Beauty standards have evolved throughout history and continue to change – what may be seen as a beauty ideal one minute can change the next (we only need to look at trends in lips to see this). It is also important to note that beauty ideals are different between cultures and races, so it is hard to pinpoint a universal ideal.
For instance, Caucasian faces tend to be narrower with greater vertical height and a pronounced 3D projection, while Asian faces tend to be wider and flatter with a shorter vertical height.
However, there are some common factors that play a part in defining what is the ideal lower third. Having a defined and streamlined jawline – a straight line from the corner of the mandible to the chin – is perceived as a sign of youth and beauty.
In women, a rounded, oval-shaped face with a well-defined chin, nice platysmal tone, good skin elasticity and a cervicomental angle that is between 90 degrees and 105 degrees with very little submental fat is an ideal shape.
In males, a more square shape with a strong chin is considered an ideal with a little bit of submental fat, but not too much. These are considered signs of masculinity.
Ageing of the lower third
Ageing is a multifactorial process and this is really important to remember. Faical ageing encompasses:
• Bone resorption
• Muscular weakness/ alterations
• Volume loss/ fat pad changes
• Skin photodamage and sagging.
When many of our patients come to us they just want to fix what they see on the surface; that’s their main concern. But for me, just treating the surface or external signs of ageing is equivalent to only looking at the tip of the iceberg – we know that what is visible on the surface does not necessarily correlate with what is actually going on underneath. I believe that unless we truly understand how the ageing process occurs and compensate for these changes at a deeper level, we won’t be successful in treating our patients.
The anatomy of the lower third
As we have already discussed, facial ageing is not due to just one factor; it is a culmination of complex processes at a deep structural level as well as on the surface of the skin. When it comes to approaching the lower third, everything starts down at the level of the bone. The bone acts as the scaffolding for everything else, so this is a very important concept.
Anatomically, the key structures at play here are the maxilla and the mandible. These bony structures serve as sca olding for all the subcutaneous tissue to produce the contour of the lower face but they shrink and change their shape and angle as we age.
Changes at the teeth level also play a role. This is because the mandible, particularly the lower mandible, acts as a platform for insertion of the lower facial musculature and ligaments. Themandibleis the largest bone in the human skull. As the lower mandible changes throughout the years all the other structures – the muscle, fascia, ligaments and even the skin – will change accordingly.
When it comes to the muscular layer, there are two important ideas. With ageing there is a partial dehiscence of muscle insertion into the fascial structures and as a result, accompanying compensatory hypertrophy of the muscles that are fixed in this area, for example the masseter muscle.
This is a very important concept as it means that those muscles are weaker in terms of their action.
The second concept, something that Dr Steve Harris has done some excellent work around, is the idea that you can myomodulate these changes that happen in the muscle with small amounts of filler. I would recommend you read Dr Harris’s article on myomodulation (AM May 2020).
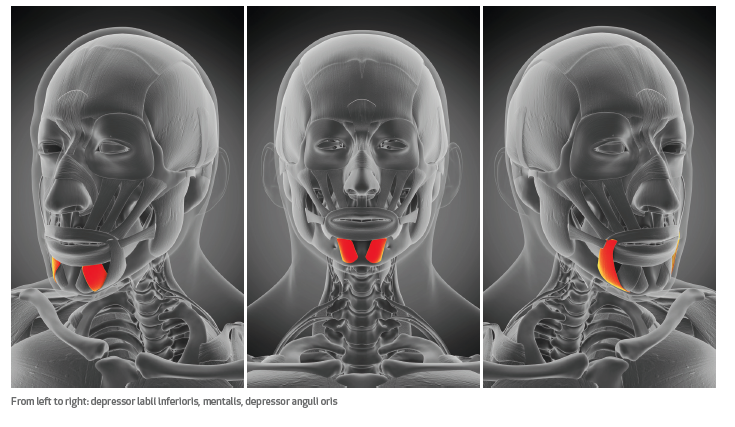
In the lower face the most important muscles are the depressor anguli oris, or DAO as as it is also referred to, the mentalis muscle and the depressor labii oris. These three muscles are very important for understanding the lower face.
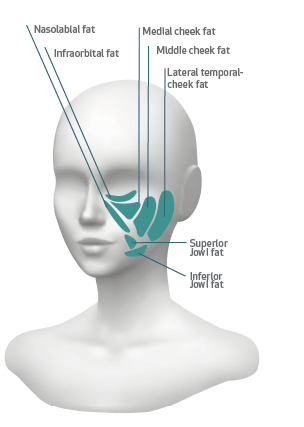
Next, we have the very well know fat compartments. When I first started practicing aesthetic medicine almost 30 years ago, we had no clue about this. This was first brought to light in a landmark paper by Rorich and Pessa and it helped us to understand the ageing process and in particular, the role of the fat compartments.
When it comes to the lower face the most important fat compartments to consider are the nasolabial fat, the superior jowl fat and the inferior jowl fat . With the loss of the fat tissue we get the formation of nasolabial folds and also the jowls which, as I stated earlier, are one of the biggest concerns for our patients.
As we can begin to see there are some landmarks we defi nitely need to consider with all our treatments of the lower face; the nasolabial folds, the masseter border, the lower mandibular line and the mandibular cutaneous ligament (which is responsible when it fails, for the appearance of the jowls), and last but not least, the submental fat.
In the second part of this article in November's Aesthetic Medicine, I will discuss my three-pillar approach to rejuvenation of the lower third encompassing volume and bone restoration, improvement of skin sagginess and dissolving submental fat.

Mr Arturo Almeida is an internationally-renowned keynote speaker, medical trainer and expert in minimally-invasive and non-surgical cosmetic procedures. A consultant surgeon, he has being practicing cosmetic medicine for more than 13 years He is a Medical Ambassador of International Plastic Aesthetic Residence (IPAR). He is based in Leeds, practicing at the VSL Clinic in Wakefield and Blemish Clinic in Manchester.

