
Let there be light
Today laser and IPL systems are used in every aspect of life for an ever increasing number of aesthetic conditions including hair removal, skin rejuvenation, acne, vascular lesions, pigmented lesions, onychomycosis and tattoo removal. The market, according to some reports, will be worth around $2bn (£1.34bn) by 2018.
LASER is the acronym for Light Amplification by Stimulated Emission of Radiation, interestingly it was originally going to be called “Light Oscillation”, which would have led to an unfortunate acronym of LOSER.
Albert Einstein first explained the theory of stimulated emission in 1917, which became the basis of laser. He postulated that, when the population inversion exists between upper and lower levels among atomic systems, it is possible to realise amplified stimulated emission and the stimulated emission has the same frequency and phase as the incident radiation. However, it was in late 1940s and 50s that scientists and engineers did extensive work to realise a practical device based on the principle of stimulated emission. Notable scientists who pioneered the work include Charles Townes, Joseph Weber, Alexander Prokhorov and Nikolai G Basov.
Despite the pioneering work of Townes and Prokhorov it was left to Theodore Maiman in 1960 to invent the first laser using ruby as a lasing medium that was stimulated using high energy flashes of intense light. In 1960, only a year after lasers were invented, dermatologist Leon Goldman began his research at the University of Cincinnati and later established a laser technology laboratory at the school’s medical centre. In 1963, he became the first physician to test the effects of this laser on human skin. It was however the theory of “selective photothermolysis” that revolutionised the medical laser Industry. In 1983, Anderson and Parrish described the theory of selective photothermolysis, which revolutionised laser therapy by explaining a method of producing localised tissue damage sparing the surrounding tissues. For understanding this we need to understand certain terms including wavelength, absorption, fluency and the thermal relaxation time (TRT) of the intended target. For tissue damage to occur a wavelength should be preferentially absorbed by the chromophore in the target tissue and not absorbed by the surrounding tissue, it therefore needs to be delivered in a pulse duration which is less than or equal to the thermal relaxation time of the target. This theory led to safer and more effective treatment procedures.
The first category of lasers to gain popularity in the UK were the CO2 laser, introduced by an Israeli company that supplied the first laser to the Albert Einstein Hospital in 1973. In the early 80s these were popular in hospitals for surgical procedures in ENT and gynaecology departments for vaporisation of tissue. The high absorption in water made them ideal for this application. It wasn’t until the introduction of micro pulsing technology, developed for char free ablation of endometriosis and such conditions, that they caught the eye of dermatologists and plastic surgeons. It soon became apparent that this technology could be used for skin rejuvenation and in the 90s people were taking years of their appearances. Unfortunately, the down time became an issue and it wasn’t until 2005 and the development of fractional technology that the CO2 lasers saw a second birth. Today this combination of very short pulse durations and and microzone injuries caused by fractional delivery heads is the gold standard for wrinkle and scar reduction.
The biggest impact however in the aesthetic laser industry came with the introduction of the first lasers for hair removal in 1994. There were two groups of scientists reporting potential results with a ruby laser for the application of hair removal. Anderson and his colleagues at Massachusetts General Hospital developed a long pulsed ruby laser and reported results on lighter skinned patients for hair removal. In the UK professor Clement, Swansea University and Dr Gault, Mt Vernon Hospital were reporting good results on skin graft patients where post excess hair became a problem on the grafted skin using the Chromos 694 ruby laser. It was actually professor Clement that got me hooked on lasers during one of his lectures, it was during one of our meetings where he showed me his bald patch from an accident with a ruby laser when he was a student.
This was something I repeated several years later, some 18 years later I still have the bald patch. The subsequent launch of this system on Tomorrow’s World saw an explosion in the UK with many companies looking to develop technology for this market sector.
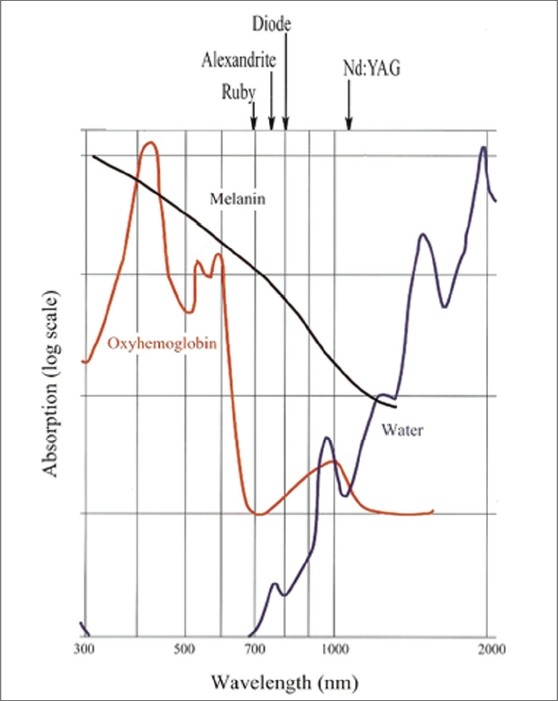
You can see from the absorption characteristics (Fig 1 left) why the ruby laser was ideal for this application, high absorption in melanin and deep penetration to target the bulb of the hair. Unfortunately, the high absorption in melanin and the short pulse duration less than 3ms meant that the laser could only be used on skin types I and II. The ruby laser was also very slow due to the combination of small spot size and a slow repetition rate.
The ruby laser was quickly followed by the introduction of the alexandrite laser, using a slightly longer wavelength of 755nm and longer pulse durations, up to 40ms, these became the industry standard for treating patients with skin types I to III. The larger spot sizes and 3Hz rep rate enabled treatments to be performed much faster than before.
This however left a gap in the market for the treatment of darker skin types, scientists started to experiment with other wavelengths and discovered that the NdYag laser (1064nm) could be effective on darker skin types. You can see from Fig 1 that the NdYag is less absorbed in melanin t
han Alexandrite so it doesn’t face the same problems on darker skins. It does however require higher energies and due to the high absorption in water is a much more painful treatment. And until recently it has been the treatment of choice for darker skin types. Another major milestone in the market was achieved when Dr Eckhouse and Dr Shraga from Israel introduced the Intense Pulsed Light (IPL) system. Unlike a laser system this emitted a wide spectrum of light from 400nm to 1200nm. Optical filters were used to block out lower wavelengths enabling the IPL to be used for different applications. One of the great advantages of the technology was the fact that the energy could be delivered through a Sapphire block enabling the operator to press into the tissue increasing the absorption of the light into the hair follicle.
The early systems were introduced to treat various vascular and pigmented lesions and later developed for hair removal. The cheaper manufacturing costs and reduced development times opened the door for many companies to enter the market and moved the hair removal business into the high street. Unfortunately, large variations in specifications meant that hair removal results were not always as good as those seen with laser systems with some clinics reporting treatments upwards of 15 treatments. For me the IPL is a great tool which is still my first choice for the treatment of fine hair and for general facial rejuvenation where the concern is redness and pigmentation. See fig 2 (below right).

I worked on an interesting theory with my colleague Dr Freeman and Dr Haziza where we looked at destroying the bulge rather than the bulb. We know that the germ cells multiply in the bulge before growing down to form the bulb. Our theory was to target the blood vessels feeding the bulge. Using a 3ms IPL with a wavelength of 500nm-1200nm we showed promising results on finer lighter hair.
DIODE LASERS
In the past few years the introduction of diode laser technology has seen the industry move towards Platform technology with various wavelengths including 808nm, 810m, 940nm, 1320nm and 1064nm available. Diode lasers possess all the characteristics of lasers but are engineered from semi-conductor plates stacked together with an optical grove to produce the lasing action. They only require a low voltage to energise them and therefore do not need the larger power supplies required for traditional laser systems.
Diode lasers are generally delivered to the tissue via a sapphire block, which can be cooled to protect the epidermis. They are small compact units that can be easily fitted into the delivery handpiece, these are taking the industry to a new dimension. One of the most recent and exciting innovations in diode laser technology is the Magma system out of Israel which combines IPL, with 808nm and 1064nm diode lasers. Interestingly one of the chief scientists behind the innovation is Dr Shraga one of the original team behind the development of the first IPL systems. This innovation allows treatment plans to be tailored to the individual patient’s requirements.
I used this for the first time seven months ago, the results have been incredible. Fig 3 (right) is a man’s back after only two treatments, treated using the 808nm diode head with a pulse width of 50ms. His first treatment was performed on an active tan.

The Magma 808nm diode laser is one of the first systems that is suitable to treat all skin types including skin type VI. This is due to its flexible pulse durations from 5ms to 400ms and chilled tip cooling system. Clinical trials in Israel showed an 86% clearance after three treatments, many UK users are reporting excellent results after only four treatments.
Platform lasers are already a reality, something which could have only been dreamt of 30 years ago. Who knows what the next 30 years will bring but, one thing is for sure, the flexibility of diode lasers will be at the heart of the next generation. The future is very exciting…

